Anatomy of visual pathways
The optic nerves assemble in the midline at the optic chiasm as shown in first figure. Here, 53% of the optic nerve fibers, those from nasal halves of the retina, cross to the contralateral part in the optic decussation. The axons from temporal halves of the retina remain on the ipsilateral side. The retinal axons leave optic chiasm to enter the optic tracts from where they go to three targets. A small proportion goes to the pretectum of the midbrain that controls pupil and accommodation reflexes. The others go to the superior colliculus in the tectum of the midbrain that organizes numerous visual reflexes, and a visual pathway runs to the hypothalamus to entrain circadian rhythms. The vast majority of axons go to the lateral geniculate nucleus (LGN) of the thalamus. From this point, the optic radiation sweeps to the medial aspect of the pole of the occipital cortex, nearly all axons terminating in layer IV of Brodmann region17, the striate or primary visual cortex (V1). The retina–LGN–visual cortex pathway is responsible for the visual perception. The visual defects characterized clinically can provide clues to the site of the lesion in the visual system as shown in the second figure.
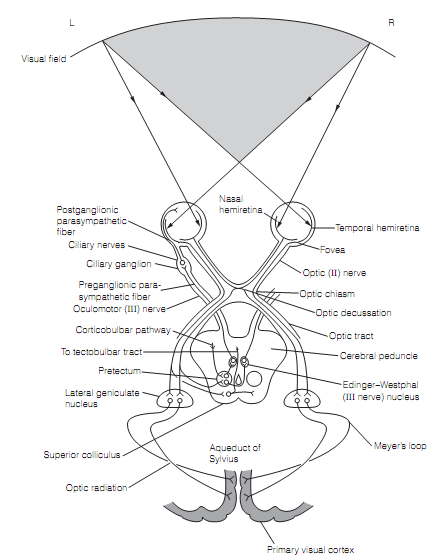
Figure: Visual pathways. Reflex pathways are shown full only on left side. Direction of the light rays from left and right halves of the visual field into the eyes is depicted. Note that the light from left visual field falls on the right halves of each retina (nasal hemiretina of the left eye, temporal hemiretina of the right eye) and light from the right visual field goes to the left hemiretinas. The binocular vision is possible only in the shaded area.
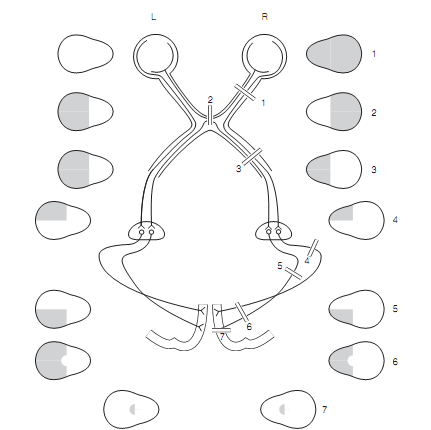
Figure: Visual defects occurring from damage to visual pathways. The lesion 2 generally arises from compression of the central section of the optic chiasm by a pituitary tumor. The optic tract lesions 3 are very rare. The optic radiation damage is generally due to an infarct or a tumor in the temporal lobe 4 or parietal lobe 5. The lesion 6 is generally caused byocclusion of the posterior cerebral artery. The fovea region is spared as it is supplied by the middle cerebral artery. The damage to one occipital lobe pole is generally caused by trauma and, as the fovea has by far the largest representation; that is the selective loss of foveal vision is typical (i.e., the lesion 7).